









.jpg?width=1024&height=576&name=vRad-High-Quality-Patient-Care-1024x576%20(1).jpg)







%20(2).jpg?width=1008&height=755&name=Copy%20of%20Mega%20Nav%20Images%202025%20(1008%20x%20755%20px)%20(2).jpg)



 Joe Schmugge
Joe Schmugge
1 min read
Trauma Awareness Month and vRad’s Impact
As I mentioned in my last post, May is both Trauma and Stroke Awareness month. vRad serves hundreds of trauma and stroke centers across the U.S. The...

Today is our third and final post in deference to Stroke and Trauma Awareness Month:
Follow the links above to our previous topics, or stick around to gain insight into the technology we use today and continue to refine for tomorrow, as we continue shaving precious minutes off the communication of critical findings.
The competing dichotomy between timeliness and accuracy is never more apparent than it is in emergency radiology, and specifically stroke protocol. Time and accuracy becomes a matter of life and death.
The National Institute of Neurological Disorders and Stroke (NINDS) outlines time segments in which stroke-combative practices must occur – simply “Critical Time Goals”. Here’s a look into the timeline set by the institute:
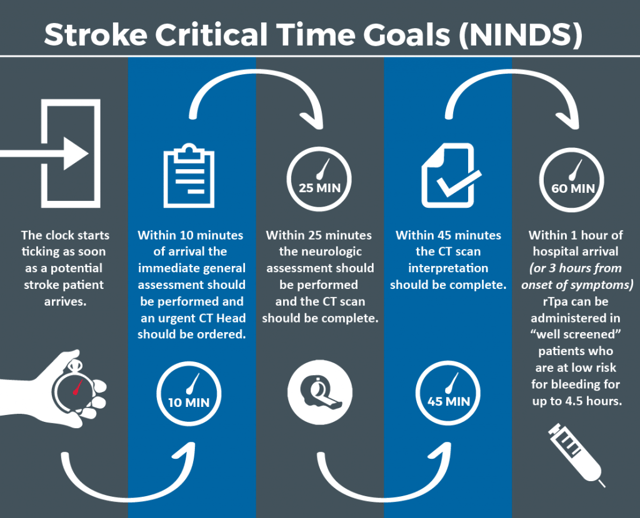
rTpa (recombinant tissue plasminogen activator) is the most commonly used drug for thrombolytic therapy. It is absolutely crucial, however, that a patient meets the requirements before the drug is given: being well-screened and diagnosed with a low risk for bleeding. For best results, the drug should be administered within 3 hours of the onset of symptoms but it is still moderately beneficial if administered within 4.5 hours.
Thrombolytics are not given to someone who is having a stroke that involves bleeding in the brain. They could worsen the stroke by causing increased bleeding.
If everything goes smoothly, we have 20 minutes once the scan is complete to interpret the images and relay our findings.
This set of guidelines drives vRad’s internal protocols, and our relentless commitment to efficiency and accuracy.
Quickly conveying critical findings is our top priority and emerging technology presents an opportunity to further enhance our ability to serve stroke and trauma patients.
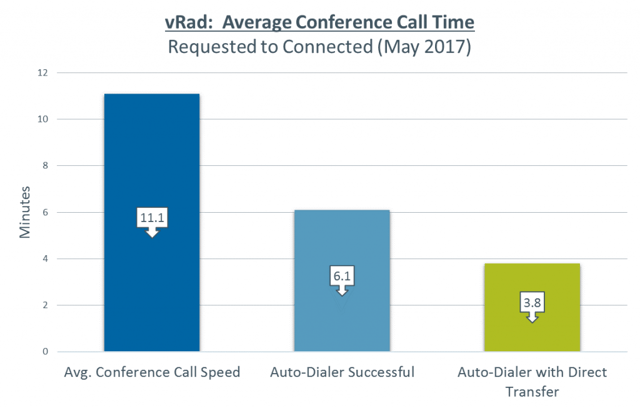
In recent years, we have developed an “Auto-Dialer” phone system that will automatically enact the process of connecting the referring physician to our physician at the point that a critical finding is detected.
When an order is submitted, we require that it include the referring physician’s name and phone number.
When our radiologist identifies a critical finding, a conference call request is automatically generated based on voice recognition of critical findings within the vRad Radiology Information System (RIS) application.
As soon as this occurs, our phone system then immediately initiates a phone call to the referring physician. (We likewise maintain the ability for a radiologist to request a conference call at the click of a button for any other reason that also immediately initiates the Auto-Dialer system)
What Happens Next…
Direct Transfer: We have the ability to activate “Direct Transfer” for specific facilities and referring physicians that are committed to providing the correct contact information and remaining available during the time we are providing coverage. When it works, this is an extremely powerful tool and we are actively looking at ways to increase the usage of this option.
vRad handles hundreds of conference calls each day and more than 190,000 critical finding conference calls annually. Currently, over 50% of all conference calls are successfully managed through the Auto-Dialer system and we continue to make investments to further improve this technology.
Artificial Intelligence. Machine Learning. Are these just buzzwords?
Not to us.
In radiology, AI is a logical next step.
Our first goal on the journey is to further support radiologists. We don’t believe AI will ever replace radiologists. We do believe artificial intelligence will help radiologists to automate identification of objective clinical information, and eliminate administrative burden. In fact, we’re already doing some of this.
Triaging critical findings, by using AI algorithms to escalate studies that are more likely to have life-threatening findings present, is the first challenge we’re taking on.
Broadly speaking, there are 3 main ingredients used to “teach” an AI system how to identify specific findings:
As the largest teleradiology practice in the country, we have the data in the form of radiology images; we have the data labels in the form of reports with findings; and we have the computer power (admittedly, with the help of a few strategic partners who specialize in the space).
The exact method used to synthesize these ingredients into an algorithm (or model) is complex, and better left to our technical teams. But operationally, the potential is exciting – and I’m thrilled to be a part of it.
I hope you’re as excited about the future of radiology as I am,
Joe

1 min read
As I mentioned in my last post, May is both Trauma and Stroke Awareness month. vRad serves hundreds of trauma and stroke centers across the U.S. The...
1 min read
A growing number of health organizations are making computed tomographic perfusion (CTP) a critical part of their stroke intervention protocols.

1 min read
Through CGI (computer-generated imagery), the folks at Pixar – creators of Finding Nemo, Toy Story, and Monsters, Inc. – allow audiences to explore...
vRad (Virtual Radiologic) is a national radiology practice combining clinical excellence with cutting-edge technology development. Each year, we bring exceptional radiology care to millions of patients and empower healthcare providers with technology-driven solutions.
Non-Clinical Inquiries (Total Free):
800.737.0610
Outside U.S.:
011.1.952.595.1111
3600 Minnesota Drive, Suite 800
Edina, MN 55435