









.jpg?width=1024&height=576&name=vRad-High-Quality-Patient-Care-1024x576%20(1).jpg)







%20(2).jpg?width=1008&height=755&name=Copy%20of%20Mega%20Nav%20Images%202025%20(1008%20x%20755%20px)%20(2).jpg)



 Benjamin W. Strong, MD
Benjamin W. Strong, MD
1 min read
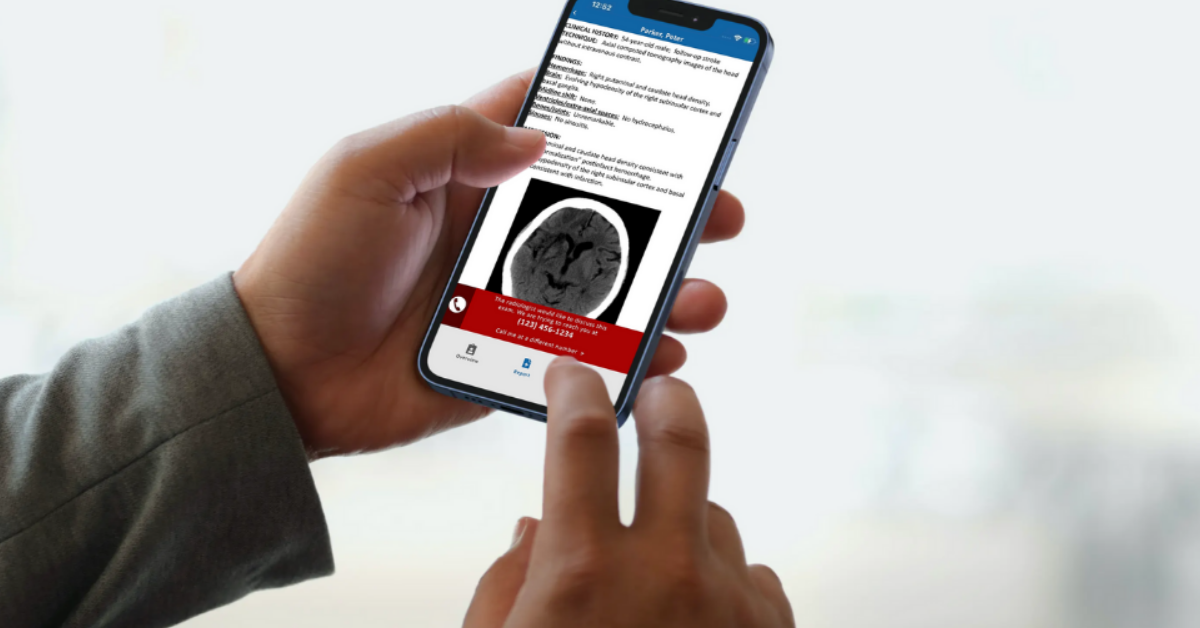
Rad Results: The Mobile App That Connects Radiologists with the Patient Care Team
Originally published by Michael Walter on Radiology Business In radiology, it is vital for radiologists to connect with the entire patient care team...
.png)
Originally published by Michael Walter on Radiology Business
Medical malpractice claims are a significant source of anxiety for all radiologists. Unfortunately, decisions made in the heat of the moment, with the absolute best intentions, can still land a specialist in court.
In my role as chief medical officer for vRad, I’m intimately involved with our radiology malpractice claims and have observed commonalities among them. To quantify these observations, I recently analyzed all 220 claims made against vRad radiologists between June 2017 and October 2020—applying a detailed classification taxonomy including the alleged type of miss, study type, if the standard of care was met, if communication failures contributed, settlement, and so on.
What emerged from that data was a clear set of guidelines to help radiologists avoid the costliest and most likely cases to go to trial.
Keep in mind, during that timeframe, our 500+ radiologists read nearly 20 million studies and logged an error rate of just 1.3 major misses per 1,000 reads—one-third the rate of the oft-cited Wilson Wong study on QA.
I analyzed vRad’s claims in great detail and formed the following prioritized recommendations for avoiding medical malpractice in radiology.
When I first started this research, I guessed that communication issues were behind one-third or even one-half of all medical malpractice cases rather than an actual missed finding. But, to my surprise, communication issues were only a factor in fewer than 12% of the cases.
We tend to see this issue pop up with acute pneumonia, which does not seem to set off the same alarm bells in a radiologist’s head as, say, an acute stroke would. But those simply must be called to the referring clinician—it is not enough to simply put it into the written report.
New diagnoses of pneumonia in an acute care setting should always result in a phone call. Failure to treat pneumonia quickly can and does result in sepsis and severe morbidity and mortality.
Around 35% of the reports issued by our radiologists are preliminaries. These are typically reviewed the next day by our client radiologists onsite before they issue a final report.
Both remote and onsite radiologists can get tangled up in legal issues with preliminary reads.
For the remote radiologist, there can be a temptation to think, “If I miss something, the next person will catch it.” The same can be said for the second reader. They may not give the study their full effort since another radiologist has already read it.
In reality, this imagined “safety net” is just not there.
Looking at the data, in preliminary studies progressing to lawsuits, approximately half of the missed findings by the initial remote radiologist were also missed by the second onsite radiologist. And the other half, where the second radiologist saw the finding, that radiologist put it in the final report but failed to call anyone about it.
Both radiologists will end up in court in these instances as preliminary status is not a defense for a missed finding, whether emergent or not.
Many practice policies and quality initiatives focus on giving radiologists plenty of background data, whether it’s prior studies, good clinical history, lab values, and so on.
What we have seen, however, is that these things were not major contributors in a single medical malpractice case. Much more important is getting access to and viewing all of the planes of imaging—meaning the axial, coronal and sagittal—and using them routinely in every study evaluation.

A lengthy report with multiple, seemingly disparate findings and no unifying diagnosis can be an indicator to the reading radiologist that greater cognitive effort is required for that particular study.
I’ve seen this most often in ischemic bowel cases, where multiple nonspecific findings such as dilated bowel loops or peritoneal fluid can be present, but the specific cause (vascular compromise) remains invisible or elusive. In these cases, it is tempting to leave things at a list of findings that are not a diagnosis and do little to help direct a clinician’s efforts. Instead, reports that amount to “notes but no music” should prompt the radiologist to return to the case in search of that unifying diagnosis.
With contrast-enhanced MRI studies, it is essential to take a specific, cognitive note of which image sequence you are looking at to avoid what I refer to as the total reversal phenomenon—an abnormal finding so extensive that it looks normal.
I see this in extensive meningeal/epidural infections and in diffuse bone marrow replacement. Extensive enhancement in meningitis can cause the gadolinium sequences of a spine or brain to look much like a normal T2 sequence, and diffuse marrow infiltration can make an abnormal T1 look like a normal T2. Taking a mental note of the exact sequence parameters you are viewing is the best strategy to avoid this issue.
Cases of missed aortic dissection that end up in court often share a few traits that explain why the radiologist didn’t see the critical finding. For example, one scenario involves studies ordered for something other than aortic dissection, making it very difficult to visualize the aorta. An abdomen study, for example, will only include the abdominal portion of the aorta in the image set. Likewise, a chest CTA done for pulmonary embolism will have intravenous contrast in an entirely different vessel than the aorta. Or, for that matter, calling an aortic dissection on a study without any contrast at all is exceptionally difficult. But it can be done.
The second common thread is an absence of clinical history to suggest aortic pathology. None of the aortic dissection malpractice cases I’ve reviewed mentioned the classic description of tearing pain between the chest and back. Instead, there were histories of flank pain common with renal stones, pain during inhalation suggesting possible pulmonary embolism, or any number of referred pains (such as neck) that can be misleading to the radiologist.
Always assess the aorta to the best of your ability, no matter the imaging parameters or reason for the exam.
That brings us to the number one thing you can do to avoid a medical malpractice suit.
Even before this recent analysis, going back to the decade I spent on our Quality Assurance Committee, I can tell you the vast majority—in fact, nearly all missed findings—are the result of failing to adhere to an established search pattern for that specific procedure.
Every radiologist should develop and follow a strict, organ-by-organ checklist for every interpretation. Know precisely what you’re going to look for, look at, and comment on.
I’ve got to look at the spinal canal. I’ve got to look at the aorta. I’ve got to look at the superior mesenteric artery. That’s a big one, by the way—the most missed single entity in all the cases I reviewed.
Adhering to your search pattern is the only way, in my opinion, to avoid those errors that the next morning are so obvious, so visually conspicuous and so avoidable.
Back to Blog
1 min read
Originally published by Michael Walter on Radiology Business In radiology, it is vital for radiologists to connect with the entire patient care team...
.png)
1 min read
At some point in your career, if you are lucky, you find somebody approachable who’s blazed trails and navigated difficulties in ways you can model....

1 min read
I love to watch the colors change in October, when pink is in full display during Breast Cancer Awareness month. With each hot-pink scarf, T-shirt...
vRad (Virtual Radiologic) is a national radiology practice combining clinical excellence with cutting-edge technology development. Each year, we bring exceptional radiology care to millions of patients and empower healthcare providers with technology-driven solutions.
Non-Clinical Inquiries (Total Free):
800.737.0610
Outside U.S.:
011.1.952.595.1111
3600 Minnesota Drive, Suite 800
Edina, MN 55435